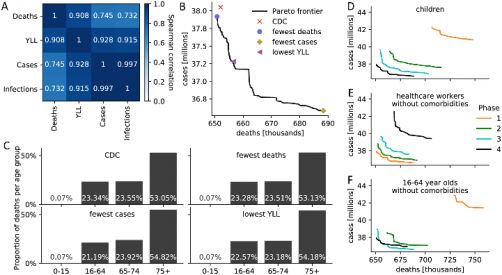
Comparison of CDC and optimal vaccine allocation strategies. (A) Spearman correlation between four measures of disease burden based on a complete comparison of all 17.5 million meaningful four-phase vaccine allocation strategies. (B) Pareto frontier of all optimal strategies based on a global search of all 17.5 million meaningful vaccine allocation strategies. For strategies on the Pareto frontier, there exists no other strategy that performs better in one objective (minimizing deaths or cases) while not performing worse in the other objective. The death and case count resulting from four specific allocations is highlighted. (C) For the four strategies highlighted in (B), the distribution of all resulting deaths across the four age groups is shown as a measure of equity. (D-F) Pareto frontiers of all optimal strategies are shown when restricting (D) children, (E) healthcare workers without comorbidities, (F) 16–64 year old without comorbidities and without an essential occupation to a certain priority phase. S8 Fig contains Pareto frontiers for all sub-populations. Courtesy of Islam et al., 2021, PLOS ONE
The four-tiered vaccine prioritization strategy implemented by the US Centers for Disease Control and Prevention (CDC), when compared computationally to all possible COVID-19 vaccine roll-out approaches, performed well by many measures but could be improved upon. The results are published this week in a new study in the open-access journal PLOS ONE by Rafiul Islam and Claus Kadelka of Iowa State University, and colleagues.
Anticipating an initial shortage of vaccines for COVID-19, the Centers for Disease Control (CDC) developed priority vaccine allocations for specific demographic groups in the population. This prioritization strategy, and its impact on subsequent disease, has been studied in many ways, but generally only compared to a small number of other vaccine roll-out strategies at a time.
In the new study, Kadelka and colleagues developed a disease model that divided the U.S. population into 17 subpopulations based on the characteristics included in the CDC vaccine recommendation—age, co-morbidity status, job type, and living situation. There are roughly 17.2 billion total ways to allocate vaccines among these 17 subpopulations in up to four phases. The researchers found that only 17.5 million can be optimal. They compared these 17.5 million allocation strategies and analyzed the resulting effect on COVID-19 cases, mortality, and years of life lost (YLL), using well-established assumptions on COVID-19 incubation and spread, vaccine hesitancy and vaccine effectiveness rates.
According to the analysis, the CDC allocation strategy performed well in all vaccination goals but never ranked the highest of all possible strategies. Compared to the respective optimal methods, the CDC approach led to an estimated 0.19% more deaths, 4.0% more cases, 4.07% more infections and 0.97% higher YLL. Note that there are tradeoffs between the vaccination goals so that no single strategy performs best in objectives: low death counts come, for example, at the expense of higher case counts. The CDC decision to not prioritize the vaccination of individuals under the age of 16 was optimal, as was the prioritization of healthcare workers and other essential workers. However, theoretical strategies which more highly prioritized the vaccination of individuals with comorbidities in all age groups were estimated to improve outcomes. The authors believe that this optimization approach can be used to inform the design of future vaccine allocation strategies around the world.
The authors add: “We developed a model that enables an accurate evaluation of the United States COVID-19 vaccine prioritization. The model further shows how the choice of optimal vaccine strategy depends on parameters such as hesitancy or how a specific vaccine functions.”